The pathologists have long since maintained that the entrance wound was "slightly above the EOP," which is about 10 cm below the HSCA placement. The HSCA noted nothing resembling a bullet entry wound is visible near the EOP in the lateral X-ray in either the non-enhanced or enhanced version. I thought it would be interesting to see if anything else on the X-ray could support or rule out the low entrance point.
The pathologists noted in the Supplementary Report to the autopsy that the brain contained a laceration across its length "approximately 2.5 cm to the right of the of the [sic] midline which extends from the tip of the occipital lobe posteriorly to the tip of the frontal lobe anteriorly. The base of the laceration is situated approximately 4.5 cm below the vertex in the white matter." The entry wound is also 2.5 cm to the right of midline, so this laceration is likely related to the passage of the bullet fragments.
The first thing to determine is where the brain's vertex (its high point) would be on the lateral X-ray. Measuring an MRI image of a skull that included centimeter markings, I found the brain's vertex to be a bit less than 2 cm below the very top of the skull. Since the top of the skull appears displaced upwards in the lateral X-ray, I overlaid it on a pre-mortem X-ray of JFK as seen below:
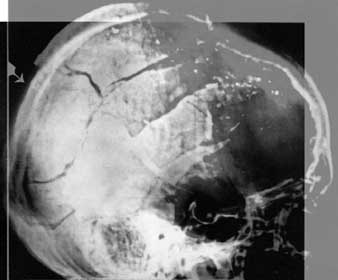
The pre-mortem skull outline shows up as a hazy gray edge on the upper right and a relatively bright white edge on the upper left (but not the very outer edge of the skull). The pre-mortem X-ray is cut off at the very top, but these contours leading up to the vertex match so we can confidently locate the top edge of the skull as the bright edge at the top of this particular image. (Follow the posterior edge of the pituitary fossa [the hook shape in the skull's center] straight up to the top of the skull. The white edge is where the top edge of the skull should be.)
Based on the HSCA radiologists' measurements, I determined that the depression fracture on the back of the skull is 10.6 cm above the point of the EOP. (See Scaling and Orienting the X-rays) I then drew a vertical green line on the lateral X-ray marking 4.5 cm below a point that is 2 cm below the skull's vertex. The lower end of this line should mark the approximate level of the base of the laceration through the brain.
Next, I drew a red line marking the low entry path through the head as maintained by Humes, Boswell, and Finck. The autopsy report states the location as "slightly above" the EOP. Barb Junkkarinen thinks this means it is about a quarter-inch above the very top of the EOP. That seems reasonable because if it were at least a centimeter, one would expect the autopsy report to include a numerical measurement here.
The bullet fragmented, so there is no single exit point for all the fragments. I chose the coronal suture as the forward-most exit point since we have photos of an outwardly beveled hole near this area, the likely result of a fragment exiting.
The red line represents the possible path of the one fragment that created the exit hole at the coronal suture.
I also marked the HSCA path in yellow.
As you can see below, the red line passes just under the base of the laceration marked by the bottom of the green line. They are probably within the range of my measurement error, though. However, if the laceration did not extend below the level of where the green and red lines (almost) meet, then the spray of fragments would have had to be confined to the area above the red line. That all the fragments would veer upward like that does not seem probable at all. One might also expect the injury to extend below the trajectory line because of the temporary cavity created by the fragment's passage.

The HSCA path, on the other hand, appears just as one would expect. The yellow line passes through the center of the green line. The fragments coming from the vicinity of the entrance point would fan out into a cone shape. (Plus, the fragments' passage creates a temporary cavity, expanding the damage.) Damage would occur above and below the centerline, the yellow line. This matches the laceration noted in the report.
Furthermore, a trail of metallic fragments is just anterior of the yellow line's arrow. They align much better with the higher entry trajectory then the lower one.
The Other Noted Laceration
The report also describes two other lacerations: "there is a laceration of the corpus collusum extending from the genu to the tail. Exposed in this latter laceration are the interiors of the right lateral and third ventricles." And viewed from below, they found, "a longitudinal laceration of the mid-brain through the floor of the third ventricle just behind the optic chiasm and the mammillary bodies." These describe the same general area which I marked on the MRI image below with a blue X.
This damage appears to be at the midline according the HSCA brain drawings. (The larger laceration was 2.5 cm to the right of midline, exactly where the entrance wound was.)
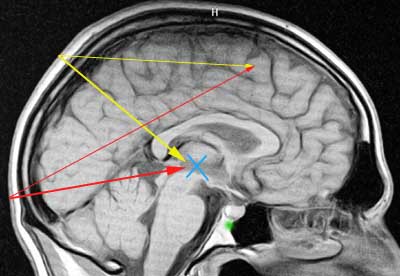
The red lines represent the low-entry trajectories. The upper red line marks the probable path of the fragment exiting at the coronal suture. Again, this line would have to mark the lower boundary of the passage of the majority of the bullet fragments since the base of the larger laceration is at the level of the white matter just below the red line at the center. The segment of the red line posterior to this point falls below the base of this laceration. This is a problem for the low-entry point.
The lower red line marks a possible path to the lacerated region at midbrain. Here, I was seeing if a fragment projectile could explain the damage. The low-entry point appears better suited to be the source of a projectile. However, this would mean the fragment passed through the cerebellum. No such injury is noted in the report, and the brain photographs rule out such injury. Also, no metallic fragments are forward of this point on this trajectory, except the 7 x 2 mm fragment above the frontal sinus. But this fragment is 4 cm to the right of midline.
The yellow lines mark possible fragment trajectories from the higher HSCA entrance point. The upper yellow line matches the extent of the larger laceration much better than the upper red line. A metallic fragment could explain the damage to the midbrain, except that no metallic fragments were noted on this path either. Bone fragments are in the left sphenoidal sinus. I marked their location with a green dot. (A fracture runs through the floor of the pituitary fossa [also called the sella turcica, the "hook" in the X-ray] so these bone fragments did not necessarily come from the entry point.).
It seems likely, then, that a spray of metallic fragments did not cause the damage to the midbrain. More probable causes are tearing related to a temporary cavity and/or the passage of bone fragments.
The Large Defect
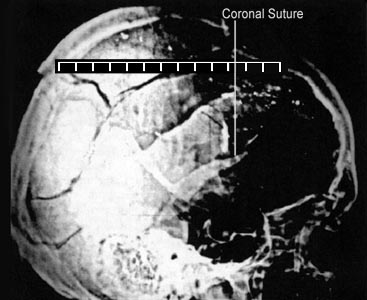
The autopsy report states the large defect on the skull measured "approximately 13 cm. In greatest diameter." It has been suggested that if the anterior margin of the defect is at the coronal suture, then 13 cm to the rear of that would extend past the HSCA proposed entry site into the occipital bone.
The graphic below shows a 13 cm ruler overlaid on the skull with the 0 cm mark at the approximate rear edge of the defect as identified by the HSCA. I located and marked the coronal suture by inspecting the pre-mortem lateral X-ray where the suture is easily visible. Also, its location above the "hook" of the pituitary fossa corresponds to the marked location of the suture in a lateral X-ray in my anatomy book.
The rear margin of the defect is a little over 10 cm behind the coronal suture. This is the measurement obtained by holding the ruler parallel to midline. The measurement in the autopsy report, however, states the length of the "greatest diameter." So if the ruler was positioned diagonally across the top of the skull, then the pathologists could very well have obtained a measurement of 13 cm. (For example, the diagonal of a square 9.2 cm on a side is 13 cm.)
(Note that I have not attempted to take into account magnification factors that result from the X-ray tube being 44 inches away from the film. The midline of the skull is probably at most 44" / (44" - 4") or about 10% larger on the X-ray. So the rear margin of the defect would be a bit more than 9 cm behind the coronal suture. Keep in mind that is for a measurement parallel to and at the midline.)